Reconstructive and
Aesthetic Surgery
The aim of plastic surgery is to restore, reconstruct or alter the human body. It can mainly be divided into two categories. The reconstructive surgery includes craniofacial surgery, hand surgery, microsurgery, and the treatment of burns. The second is cosmetic or aesthetic surgery.
Reconstructive Surgery
After trauma, cancer or congenital malformations the plastic-reconstructive surgeon is able to correct skin and subcutaneous tissue, muscle, tendons, nerves and bones and cartilage by transplantation of human tissues within the same body and between different human beings (face transplant). The tissue is either transposed or rotated locally as a pedicled flap or detached from his vascular bed and reattached by the use of very precise small instruments and microsurgical techniques.
to be continued...
The development of the perforator flaps lowered the donor side morbidity and facilitated more aesthetic results. The improvement of the microsurgical techniques dropped the vascular complication rate dramatically (< 1% for autologous breast reconstruction). Therefore the formerly reconstructive ladder principle is not continued anymore. Today we choose the individual best option.


Hand Surgery
The hand represents only a small part of our body but has an enhanced number of highly developed functions. Think only about the craftsmanship and creative abilities, our hands offer. The function is only possible through the close interaction of the anatomical structures (bones and tendons, tendons and muscles, vessels and nerves). Therefore the hand is a highly complex organ, which is most time unprotected and therefore predestined for injury.
to be continued...
Today hand surgery is a subspeciality of surgery, orthopedic surgery or plastic surgery. Hand surgery became a part of the plastic surgery training mostly by providing an atraumatic surgical technique. A technique enabling an extremely low impact of tissue is mandatory for the conservation of these small anatomical structures. In most countries plastic surgeons were the first surgeons performing replantations of fingers and hands.
Microsurgery
Contemporary reconstructive microsurgery was introduced by an American plastic surgeon, Dr. Harry J. Buncke. First he reported the successful anastomosis of a 1 mm blood vessel in a rabbit ear replantation and 1966 the replantation of a primate’s great toe to its hand. The first human microsurgical transplantation of the second toe to thumb was performed in February 1966 by Dr. Dong-yue Yang and Yu-dong Gu, in Shanghai China. After this successful reports many free tissue transfers were developed and published. Free tissue transfer is a surgical reconstructive procedure using microsurgery. A region of “donor” tissue is selected that can be isolated on a feeding artery and vein; this tissue may include several tissue types (skin, muscle, fat, bone,…). The tissue is transferred (moved as a free flap of tissue) to the region on the patient requiring reconstruction. The vessels that supply the free flap are anastomosed with microsurgery to matching vessels (artery and vein) in the reconstructive site. In the last years the development of perforator flaps reduced the donor site morbidity and allowed more aesthetic pleasing reconstruction results.
A microsurgical treatment might
reattach amputated body parts (replantation)
transplant tissue from one part of the body to another (microvascular transplantation)
repair nerves
repair blood vessels
manage complex soft tissue and bone infections


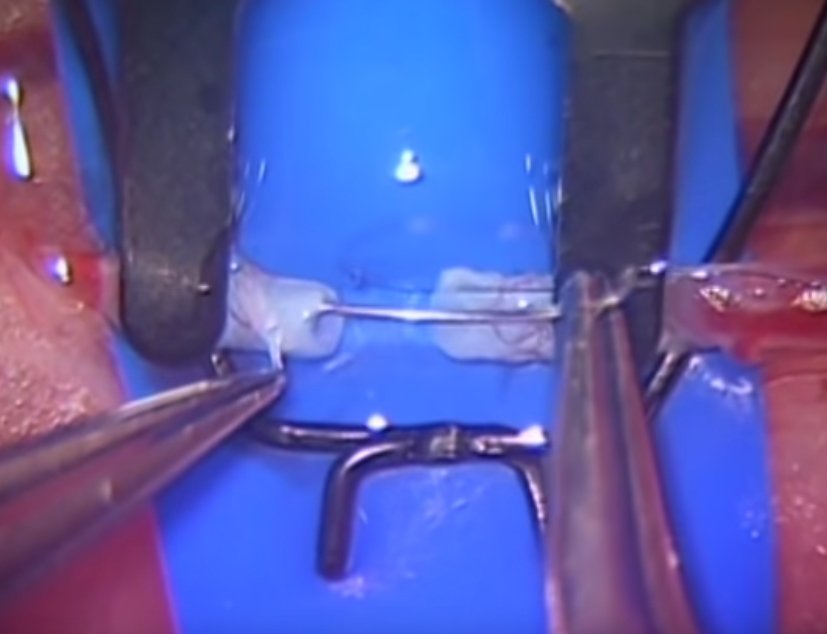
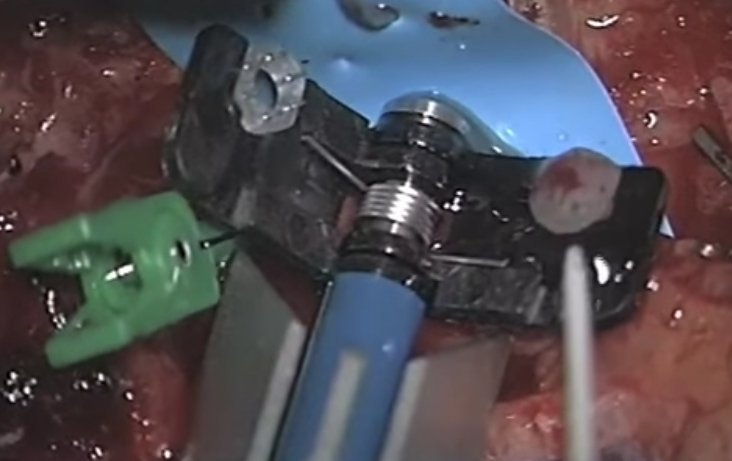
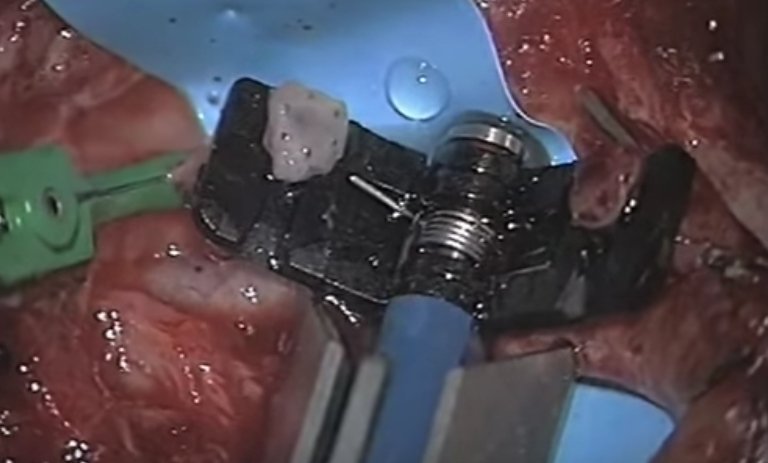
Pictures:
Left row up: End-to-side anastomosis
Left row down: microsurgical instruments
Right row up: End-to-end anastomosis
Right row middle: venous anastomosis with sillicone device
Right row down: second vessel wall is everted and impaled on the pins
A microsurgical treatment might
reattach amputated body parts (replantation)
transplant tissue from one part of the body to another (microvascular transplantation)
repair nerves
repair blood vessels
manage complex soft tissue and bone infections

Guidelines to transfer to Burn Center:
Partial thickness burns >= 20% Total Body Surface Area (TBSA) in patients aged 10 – 50 years old.
Partial thickness burns >=10% TBSA in children aged 10 or adults aged 50 years old.
Full-thickness burns >= 5% TBSA in patients of any age.
Patients with partial or full-thickness burns of the hands, feet, face, eyes, ears, perineum, and/or major joints.
Patients with high-voltage electrical injuries, including lightning injuries.
Patients with significant burns from caustic chemicals.
Patients with burns complicated by multiple trauma in which the burn injury poses the greatest risk of morbidity or mortality. In such cases, if the trauma poses the greater immediate risk, the patient may be treated initially in a trauma center until stable before being transferred to a burn center. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols.
Patients with burns who suffer inhalation injury.
Patients with significant ongoing medical disorders that could complicate management, prolong recovery, or affect mortality.
Hospitals without qualified personnel or equipment for the care of children should transfer children with burns to a burn center with these capabilities.
Burn Injury in patients who will require special social/emotional and /or long-term rehabilitative support, including cases involving suspected child abuse, substance abuse, etc.
(Recommendations from the American Burn Association and the American College of Surgeons)
Burn
A burn is a type of injury to skin, or other tissues, caused by heat, cold, electricity, chemicals, friction, or radiation. Burns that affect only the superficial skin layers are known as superficial or first-degree burns (1st degree, red without blisters, dry, painful). When the injury extends into some of the underlying skin layer, it is a partial-thickness or second-degree burn (2nd degree superficial, redness with clear blister, blanches with pressure, moist, very painful; 2nd degree deep, yellow or white, less blanching, may be blistering, fairly dry, pressure and discomfort; 3rd degree, stiff and white/brown, no blanching, leathery, painless; 4th degree, black, dry, painless). Scarring occurs from 2nd burn degree on. Full-thickness burns usually require surgical treatments (skin grafts, flaps,…). Extensive burns require an intensive care treatment in special burn centers.
Guidelines to transfer to Burn Center:
Partial thickness burns >= 20% Total Body Surface Area (TBSA) in patients aged 10 – 50 years old.
Partial thickness burns >=10% TBSA in children aged 10 or adults aged 50 years old.
Full-thickness burns >= 5% TBSA in patients of any age.
Patients with partial or full-thickness burns of the hands, feet, face, eyes, ears, perineum, and/or major joints.
Patients with high-voltage electrical injuries, including lightning injuries.
Patients with significant burns from caustic chemicals.
Patients with burns complicated by multiple trauma in which the burn injury poses the greatest risk of morbidity or mortality. In such cases, if the trauma poses the greater immediate risk, the patient may be treated initially in a trauma center until stable before being transferred to a burn center. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols.
Patients with burns who suffer inhalation injury.
Patients with significant ongoing medical disorders that could complicate management, prolong recovery, or affect mortality.
Hospitals without qualified personnel or equipment for the care of children should transfer children with burns to a burn center with these capabilities.
Burn Injury in patients who will require special social/emotional and /or long-term rehabilitative support, including cases involving suspected child abuse, substance abuse, etc.
(Recommendations from the American Burn Association and the American College of Surgeons)
Aesthetic Surgery
Cosmetic surgery is performed to reshape normal structures of the body in order to improve the patient’s appearance and self-esteem. Cosmetic surgeries are considered “elective.” Aesthetic surgery is part of the training to become a board certified plastic surgeon. A plastic surgeon needs to accomplish a 6 year residency in an accredited plastic surgery program or a 2-year accredited general surgery residency, followed by a 3-year accredited plastic surgery residency. Complex reconstructive surgery is the best school for aesthetic surgery. Well-qualified cosmetic surgeons are true, board certified plastic surgeons who have completed additional, fellowship training for cosmetic procedures. In Belgium the INAMI number, finishing with -210, shows the qualification of a board certified plastic surgeon.
to be continued...
Be aware of wrong use of medical titles. In addition, there are a number of agencies who claim to offer “board certification”. Unfortunately for many patients, any licensed doctor may perform “cosmetic surgery” procedures for which he is not really qualified. Not only have these patients received substandard care, they may have been placed in jeopardy and some cases of death have even been reported because of lack of training and improper practices. Do not let yourself be blinded by low fees. The bitterness of poor quality remains long after the sweetness of low price is forgotten.

Patient Information
Our patients are often overwhelmed by a waterfall of uncontrolled information offered through the media and internet. Even with medical know-how the choice of information is sometimes difficult. At the following link you can download some patient information from different scientific societies. They are written for patients in a comprehensive manner. I advise to read this information before the consultation, it will help you to follow my explanations and advise. The information forms do not replace a consultation. A consultation with a board certified plastic surgeon is crucial to succeed the treatment.
Links to scientific societies
International Society of Aesthetic Plastic Surgery (english, french, spanish,…)
Société Française de Chirurgie Plastique Reconstructrice et Esthétique (french)
Nederlandse Vereniging voor Plastische Chirurgie (Dutch)
Deutsche Gesellschaft der Plastischen, Rekonstruktiven und Ästhetischen Chirurgen (German)